

Summary:
Several years ago UnitedHealthcare launched a Consumer Resolution Center that combines AI insights with human judgment to proactively identify customers in distress and empower skilled employees to resolve their problems quickly. Working across functions and without excessive bureaucracy, CRC teams have since turned service recovery into a source of learning that has enabled the company to rewire processes, policies, and benefits at scale. The story of the CRC’s success shows how effective managers can stay close to frontline reality, trust data over intuition, and move decisively to scale what works.
A few years ago, the senior leaders at UnitedHealthcare (UHC), the insurance arm of UnitedHealth Group, asked a simple question: What if we proactively identified the customers having the most trouble with their claims and mobilized around them quickly, intentionally, and with real accountability? The best organizations know how to move fast and remove roadblocks when it matters the most. So why couldn’t we do the same for our members in distress—and just as important, use everything we learned from helping them to improve service for others?
That’s how our Consumer Resolution Center (CRC) began. Using a combination of AI algorithms and well-trained, empathetic employees, we’ve since delivered high-touch problem-solving service to 150,000 UHC members, moving their average satisfaction ratings from zero to 8.8 out of 10. We’ve also ferreted out the root causes of their problems and developed and scaled solutions that have reached more than 5 million customers, or roughly 10% of our base. The CRC, now staffed by some 330 people, has recouped the $20 million to $25 million we invested in it—many times over—through reduced inefficiencies, cost savings, and increased customer retention.
My predecessor, the late Brian Thompson, affectionately known to us as BT, was passionate about the CRC project from its inception, because his North Star was serving customers. That’s why his being killed in December 2024—and the public criticism of UHC and other health insurers that followed the tragedy—was so painful. Yes, there is much room for improvement in the ways our company, our industry, and U.S. healthcare in general are run. But our mission at UHC is to do all we can to make the system work better for everyone by rolling back unnecessary requirements and improving affordability wherever possible—and no one pursued those goals with more heart than BT.
The story of how we created and deployed the CRC is a testament to the purpose-driven culture he helped to create. It is a case study in how to leverage both technology and human talent to better serve customers—and how to scale those solutions. This is the approach we’re taking across all of UnitedHealth Group. We hope that other organizations can learn from our experience.
Stepping Up After a Tragic Loss
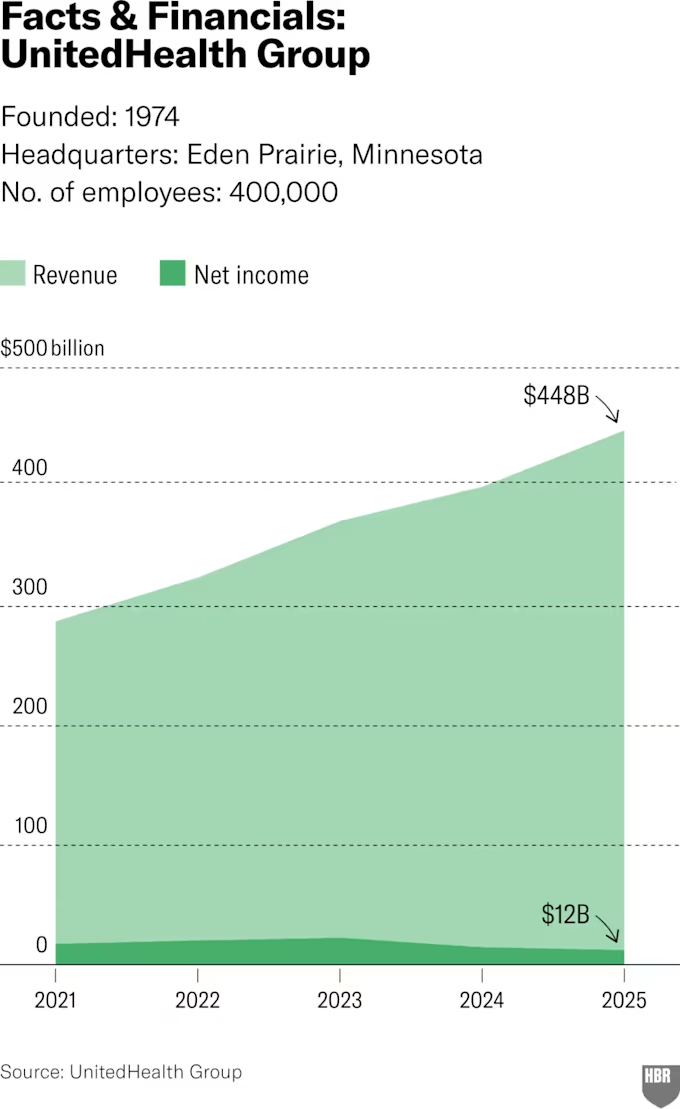
Our company was founded in 1974 as Charter Med and restructured as UnitedHealthcare in 1977. After a 1984 IPO we expanded through acquisitions to become the largest U.S. health insurance company, serving more than 50 million people worldwide. As one of UnitedHealth Group’s two divisions (medical services provider Optum is the other), we offer employer-sponsored, individual, family, and marketplace plans; Medicare coverage and group retiree services; Medicaid, Dual Special Needs, and Children’s Health Insurance Program coverage; and plans in more than 100 countries. Last year we grew revenues by 12% to $447.6 billion, from which we generated $19 billion, or about 4%, in earnings. I know that critics often question whether for-profit health insurers should even exist. My response is that our margins are capped and heavily regulated, well below the double-digit figures posted by many pharmaceutical companies and healthcare systems, and in line with what any company pooling and covering risk needs to operate responsibly.
Nearly two decades ago I came to UHC from the airline industry—another business in which service is key and unhappy customers can be extremely vocal. I was keen to join a thriving organization in my hometown of Minneapolis, drawn to the company’s goal of making healthcare more affordable, and excited about the innovation in senior care it was then pursuing. I worked my way up in our Medicare and Retirement division and led it until BT’s death.
When the board offered me his role, it was hard to imagine stepping into it. But I decided to take the job for three reasons. First, I had lost not only a colleague and boss but a mentor and close friend, and I wanted to honor him. Second, despite UHC’s size and 100,000-strong workforce, it feels like a close-knit family to me, and as one of its senior leaders I knew I had a responsibility to our team and those we serve to maintain continuity. Finally, because of initiatives like the CRC and other tech investments, I believed we were on the verge of a revolution in our ability to ensure members get great care with much less frustration, and I was determined to see that process through.
When Individual Needs Collide with a Rigid System
UHC pulled together the team that would become the CRC in 2023 to address a fundamental tension in our industry: While our members each have unique care needs, emotions, and stressors, they all must navigate a rigid system of regulatory constraints, employer-defined benefits, and clinical guidelines. As the largest U.S. insurer, handling 85 million customer interactions annually, we tend to bear the brunt of any frustrations that arise. Some of them are justified; we are not perfect, and we make mistakes. But many coverage delays and decisions actually come down not to us but to the plan the employer or government has selected—we simply execute on that contract. And even when we manage tens of millions of claims seamlessly, the ones that hit roadblocks invariably cause distress—and sometimes an uproar when people have a poor outcome that becomes public, such as an astronomical cost or a lack of coverage for experimental but potentially life-saving medicines.
Our first goal was to develop a system to identify and tackle those obstacles more quickly—what’s known as service recovery. We assembled a group of our best technologists and customer service reps—people with high emotional intelligence and deep expertise in all our offerings as well as those of external stakeholders. Then we granted them the authority to offer immediate relief, such as reimbursements or expedited approvals and referrals.
The newly formed CRC developed an outbound capacity: finding members who were struggling to navigate our system but hadn’t called us about it. The group’s technologists used AI to analyze 100 million recorded calls and identify the factors that most often lead to distress. That data was used to program a proprietary algorithm, which today continuously scans for more than 20 signals across every single member interaction (calls, website visits, emails, and more).
We proactively identify the people in greatest need, often ones facing complex or unresolved issues and who are angry or upset. Then our consultants reach out by phone to work one-on-one with these struggling members to find solutions. Our staff’s cold calls are answered a whopping 70% of the time—a good sign that we’ve correctly diagnosed a need for help. And as our improved satisfaction averages show, this VIP treatment works, turning our biggest detractors into UHC promoters.
In 2024 we added a complementary team, Consumer Operations Vitals and Experience (COVE), located at our Minneapolis headquarters. It’s tasked with monitoring consumer-facing operations and identifying real-time member issues through signals like call spikes, digital errors, and sentiment. This team rapidly coordinates fixes—often within hours—by centralizing communication, surfacing root causes, and supporting critical-response protocols, which prevents service disruptions, accelerates issue resolution for thousands of members, and further shifts the organization from reactive to proactive experience management.
Over time, we’ve beefed up our training with a tailored onboarding program, codesigned with learning experts, to teach best practices in critical thinking and conflict resolution. We’ve also continued tweaking our algorithm to ensure it keeps directing us to the most pressing customer pain points.
Turning Customer Distress into Operational Insight
The best part about today’s CRC, however, is that it doesn’t stop at helping individual members. It also uses those interactions to understand the source of each problem and fix it so that we have fewer issues in the future—what we call rewiring the system. In two years this work has driven hundreds of improvements in process, policy, and benefit design, each informed by AI and our consultant interactions and executed through cross-functional collaboration.
For example, one member’s denied claims revealed that a back-end error had misclassified an in-network provider. Fixing it led to reprocessing and accurately reimbursing 5,000 additional claims. In another case, when the CRC found that a member’s heart surgery had been postponed because of a missing digital referral (the provider had instead sent one via fax and mail), the team partnered with colleagues in our clinical coverage review department to create a new provider education and authorization process. CRC’s work with a patient needing treatment for cystic fibrosis led us to add Relizorb, a single-use digestive enzyme cartridge, to our approved treatment list because it was the best option. And calls with more than 20 members needing more dentures than they were allowed under their policies pushed us to increase the limit and add a centralized support team for the issue. We’ve also used learnings from the CRC to influence external stakeholders; for example, we persuaded one client to change ostomy supply benefits for its employees and another to expand its benefits to include often-overlooked expenses such as wigs for cancer patients.
Cases like those often require input from multiple teams, so the CRC is empowered to mobilize people across functions and business lines, accelerate decision-making, and encourage road map reprioritization where necessary. The group’s success has made it both a magnet for talent within UHC (Who doesn’t like solving problems?) and a point of pride across our entire workforce as it spurs organization-spanning innovation.
What Other Complex Organizations Can Learn
Though our expertise is in health insurance, we think the recover-and-rewire model can work for any service organization facing complexity, regulation, and high-stakes customer interactions. Implementing it starts with using frontline employees, consumer listening tools, and data to identify friction. Leaders—from middle management to the C-suite—shouldn’t sit in their offices and trust their gut. They need to create teams and systems, as we’ve done with the CRC, to get as close to the action as possible. That’s where you find the challenges you must overcome to be successful and the opportunities you can seize to innovate and grow.
Executives must also empower their people to act on what they’ve learned, whether it’s a specialized support consultant offering a refund, a manager authorizing a process or policy change, or a division head investing in a new initiative. At UHC we give team members great autonomy and flexibility to do what’s right within their domains.
Finally, members of senior management must be willing to commit to scaling meaningful initiatives quickly. Of course, like any company UHC has a robust capital-investment approval process. But we don’t have a lot of red tape when it comes to making bets on projects aligned with our strategy and mission. With technology moving as fast as it does today, pilots can be a barrier to progress. It’s important to be courageous about embracing continuous, wide-scale improvement based on the best evidence you have.
UHC has suffered several shocks over the past few years. When the Covid pandemic hit we had to quickly ramp up claims processing to meet skyrocketing healthcare demands, as well as develop the capability to help the U.S. Department of Health and Human Services deliver CARES Act relief funding to providers. Since then our employees and the communities in which we operate have faced a series of difficult events—from moments of deep social tension to heartbreaking tragedies and threats to community safety. Those challenges have affected us in many ways, and through it all we have come together to support one another and remain focused on serving those who depend on us.
Like everyone, we at UHC are looking for bright spots. We’ve found one in our work easing patients’ path to affordable healthcare. In a world of fragile trust we remain committed to building our business in a way that truly delivers on that mission and turns our worst critics into our best advocates.
Copyright 2026 Harvard Business School Publishing Corporation. Distributed by The New York Times Syndicate.
Topics
Economics
Payment Models
Strategic Perspective
Related
The Collaboration Imperative: Why Healthcare Executives Must Unite Against an Existential ThreatThe Market for Physician-Researchers’ Labor: Unpaid Work, Paid AccessFollow the Money: A Health Plan Insider’s Guide to Payer–Provider Contracting