
Healthcare organizations (HCOs) are under tremendous financial, workforce, and societal pressures to deliver safe and effective care, and have increasingly turned toward integrating physician leaders into decision-making within their organizational structure.(1)
At the same time, progressive HCOs recognize that physicians lack proscriptive leadership development in their early clinical years and HCOs must consider how best to approach physician leadership development to achieve their intended aims of physician leadership integration. HCOs therefore choose to implement myriad leadership programs to close this gap and create alignment within the organization.
What remains open for discussion, however, is how HCOs invest in physician leaders to perform specific roles within their organization. Importantly, the chief medical officer, as the senior physician leader, is critical in leading any healthcare organization.
Previous research has shown that, over the course of the program, inter-professional leadership development programs lead to increased affective commitment and a shared vision toward the parent HCO. The results suggest that participants’ shared vision of the organization and their sense of emotional attachment to it increased.(2)
Together, these two measurements suggest that, following a well-defined leadership program with outcome-based goals, participants become more committed to the parent organization that hosts and sponsors the program. This finding aligns with widely held beliefs that leadership development programs are typically organization-dependent and focus on developing leadership traits and improving contributions specific to the industry and organizational culture.
Sheri-Lynne Leskiw and Parbudyal Singh suggest that the design of any truly effective leadership development program must consider and incorporate six factors: a needs assessment, combining the right audiences in the program, infrastructure to support the development, the implementation of a learning system that will drive the individual programs, a means to evaluate the change, and actions that will reward success.(3)
If leadership development programs are hosted and executed by the parent HCO organization (i.e., organization-dependent), one challenge for the host is the potential for bias and changes in attitudes stemming from the parent organization’s involvement.
Our prior research made it clear that the inter-professional leadership development program was not intended or designed to create increased notions of shared values or affective commitment, much less any increased level of trust, but the program delivered an unintended change in those attitudes, perhaps by the location, the approach and style of the teacher, and the selected participants rather than through any rational design that could be replicated.
Also, two curriculum elements consisting of an “extraordinary experience” or field trip and a panel discussion with the parent organization’s C-suite members during the final class may have exaggerated the local nature of the program and unintentionally influenced the results.(2)
To further explore how leadership development programs influence attitudes toward HCOs, this study sought to measure four specific changes (i.e., leader self-efficacy, collective orientation, shared vision, and organizational commitment) in participants’ attitudes following a non-parent, non-healthcare organizational program for rising and early-career physician leaders.
This study provided an opportunity to determine whether leadership development disconnected from the physician participant’s parent organization and isolated from other physicians of that same parent HCO imparts changes in the physicians’ attitudes toward their own respective organizations. The results demonstrate a significant improvement in three out of four attitudes following the program’s conclusion.
As physician leadership development (PLD) programs increase across healthcare ecosystems, organizations are challenged to determine the outcomes and ascribe values to participants, much less to the parent organization. However, a growing body of evidence is beginning to emerge. Previous work demonstrated improved collaboration among physicians, nurses, administrators, and their employing organizations as a result of interprofessional programs.(4) Outcome-based and interprofessional training programs, which generate and drive specific learning objectives for individuals and teams, have proven to be an effective method to achieving productive results.(5)
Physician leadership development program evaluations most often emphasize participant reactions and self-reported learning/behavior change; however, post-course measurement of participants’ attitudes toward their organization (e.g., organizational commitment, shared vision, collective orientation) is reported far less consistently.(6) At an organizational level, this leaves HCOs to speculate if there is value in promoting PLD programs to generate these desired organizational outcomes.
As previously reported, physicians have lower organizational commitment (OC) toward HCOs, and there is potential to increase OC among physicians within an HCO following leadership development.(1,2) Amid sustained resource pressures, however, HCOs face increasing difficulty in allocating the resources required to support physician-focused leadership development, which may create structural barriers to improving organizational attitudes and leader self-efficacy.
Consistent patterns suggest that higher levels of OC among physicians are associated with favorable outcomes, such as improved care quality and productive work behaviors.(7) As such, HCO executives are faced with two questions: 1) Can the organization afford to conduct physician leadership development, or 2) Can the system afford NOT to engage in physician leadership development?
Depending on the answers, executives are next faced with decisions about how best to organize their specific program. As organizations seek to use PLD to generate organizational commitment, questions may arise about the program design (inter-professional or physician-specific), the selection process for participants, and the desired outcomes.
While physicians as primary stakeholders in healthcare organizations are most likely to be key agents of change, and while leadership development is critical to the growth of change agents, organizational success may also depend on manifesting principal physician leaders with the required skills, knowledge, and abilities (SKAs) to drive change within the HCO upon program completion.
Further, if HCOs are not equipped to develop organization-specific programs at scale, there may be a rationale for outsourcing the leadership development of their key physician leaders, namely chief medical officers (CMOs). It would then be incumbent on the CMO to return home with improved leadership attitudes and to foster and lead ongoing local physician development to achieve organizational objectives.
The CMO role within community healthcare delivery systems (e.g., hospitals and clinics) is indispensable but is often characterized by variable scope and responsibilities.(8,9) Further, the CMO is expected to be the key leader executing organizational objectives that depend on physician alignment. But given the paucity of role-specific CMO training/development programs in the United States, it is not surprising that physicians selected to serve in the CMO role lack the skills and development to lead HCOs as anticipated.
Evidence suggests CMO leadership capability is often acquired through variable, informal pathways, while PLD programs frequently report individual-level gains at completion, but less consistently report participants’ post-course attitudes toward their organization.(7,8) Nor have any known role-based PLD program researchers measured if the programs deliver the desired organizational leadership attributes.
This study investigates whether a C-based (i.e., CMO) physician leadership program produces measurable changes in participants’ organizational alignment related to leading physicians and sustaining organizational resilience and outcomes. The authors conclude that physician leaders’ organizational attitudes improve after an outsourced role-based physician leadership development program.
DESCRIPTION OF THE PHYSICIAN LEADERSHIP DEVELOPMENT PROGRAM
This study was conducted with physicians in leadership roles from multiple HCOs across the United States and Saudi Arabia. The program was labeled as a CMO Academy and consisted of live sessions at remote locations (away from the participant’s own HCO), as well as virtual sessions, conducted over 12 months. The program’s executor previously researched an inter-professional leadership development cohort and measured change in shared vision and organizational commitment. The research conducted for this role-specific physician-only program was designed to measure leadership self-efficacy, collective orientation, organizational commitment, and shared vision.
Participants in this research were members of the inaugural cohort of the American Association for Physician Leadership (AAPL) inaugural longitudinal CMO Academy. They consisted of self-selected participants in management positions preparing for a CMO role and “seeking to deepen their knowledge of management to be successful leaders in the healthcare industry.”(10) The prerequisite for participation was that the physician be in a titled formal HCO role (including, but not limited to, the CMO role) with no more than five cumulative years in their position(s).
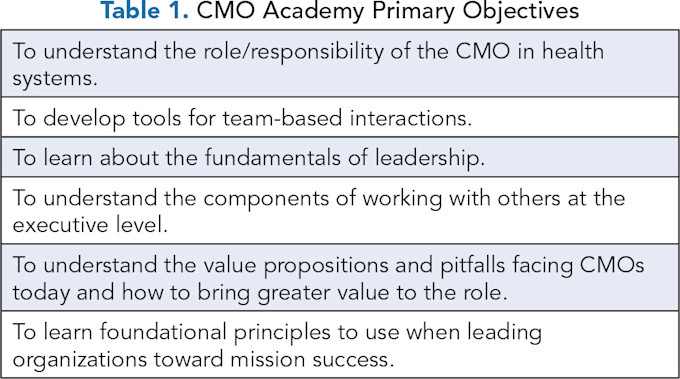
The program was designed (and marketed) to provide participants with a foundational understanding of the requirements of leadership, a deepened awareness of the complexity of today’s healthcare landscape, and additional role-specific skills and knowledge necessary for CMOs to affect organizations. The primary objectives are shown in Table 1.
The cohort participated in a course consisting of three two-day live, in-person seminars, evenly distributed over the 12 months, interspersed with virtual, in-person sessions and self-directed modules. The two-day in-person seminars included eight hours per day filled with a mix of didactics, case studies, interactive experiences, simulations, and a capstone presentation.
Each in-person seminar was led by a single instructor but also included guest speakers and adjunct attendees who provided brief (<1 hour) leadership presentations based on their roles, which allowed follow-up question-and-answer periods. Virtual meetings were led by the same principal instructor, lasting 90 minutes per session and including scenario-based case studies and breakout rooms for team interactions.
Before the start of the course, each participant engaged one-on-one with a program delivery specialist to review the anticipated program, the overall objectives, and the course requirements for earning their course certification.
At the first in-person meeting of the course, each participant received their own workbook and the books required for the program, a review of attendee responsibilities, and a second review of the course objectives and requirements for graduation/certification. Before each session, whether live or virtual, the instructor outlined the material, objectives, and expected outcomes for that session.
The course was designed to create alignment and continuity across the entire learning experience. Every session and each element of the course followed the “spiral curriculum,” revisiting concepts with increasing depth.(11) Every didactic lecture, reading, exercise, or activity had a clear downstream purpose, culminating in a capstone experience to assess their preparation for leading in healthcare (see Figure 1).

The program was built to deliver core leadership competencies, including self-awareness (self-management), leading teams (team building and teamwork), and leading others (organizations). Further, the program delivered critical management skills required to succeed as a CMO, including clinical quality improvement, risk management, regulatory compliance, financial management, leading through influence, managing competing priorities, negotiation, strategic planning, innovation, and value proposition development.
The capstone involved the student’s formal display of self-selected competencies (from a rubric of options) and skills at the end of the course to determine whether the student had absorbed the course objectives.
METHODS
A pre- and post-survey design was used to assess the extent to which leader self-efficacy, collective orientation, shared vision, and organizational commitment increased following participation in the CMO Academy program. Using Qualtrics, both surveys were designed to be identical and contained the focal study measures along with key demographic information (i.e., age, gender, race, ethnicity, organizational role, and tenure).
The Institutional Research Board at the Florida Institute of Technology reviewed the study, granted exempt status, and provided a certificate of clearance for human participants research (IRB Number: 24-187). Informed consent was obtained via the first item in the survey, and participants continued only if they selected “I consent.” Participants were informed that the survey was anonymous and that they could withdraw at any time.
The pre-survey link was sent to all participants in the CMO Academy program before the start of the course, and the post-survey link was provided on the last day of the course. The course instructor encouraged program participants to complete the surveys on the last day of the course.
Leader self-efficacy, defined as confidence in one’s ability to be an effective leader, was measured using five items taken from Ladegard, et. al.(12) Example items include “I feel confident when I make decisions” and “I am well aware of the strengths I have in my job as a leader.” All items were rated on a 5-point scale ranging from 1) strongly disagree to 5) strongly agree, such that higher scores reflect a higher level of leader self-efficacy.
Collective orientation, defined as “the propensity to work in a collective manner in team settings,” was measured using the affiliation sub-dimension from the Driskell measure.(13) Example items include “I find working on team projects to be very satisfying” and “For most tasks, I would rather work alone than as part of a group” (reverse coded). All items were rated on a 5-point scale ranging from 1) strongly disagree to 5) strongly agree, such that higher scores reflect a higher level of collective orientation.
Shared vision, defined as the extent to which the participants understood and shared the vision of the organization, was measured using four items adapted from Chai.(14) These items assessed the extent to which the participants understood and engaged with the organization’s vision. An example item is “I fully understand the meaning of my organization’s vision and mission and can fully explain it in detail.” All items were rated on a 5-point scale ranging from 1) strongly disagree to 5) strongly agree, such that higher scores reflect a higher level of shared vision.
Organizational commitment, defined as the sense of emotional attachment to the organization, was measured using seven items adapted from Chai as well as McGee and Ford.(14,15) These items assessed the extent to which the participants are attached and committed to the organization. Example items include “My organization has a great deal of personal meaning for me” and “I do not feel a strong sense of belonging to my organization” (reverse coded). All items were also rated on a 5-point scale ranging from 1) strongly disagree to 5) strongly agree, such that higher scores reflect a higher level of affective commitment. All analyses were performed using SPSS Statistics Version 28.0.1.1.
RESULTS
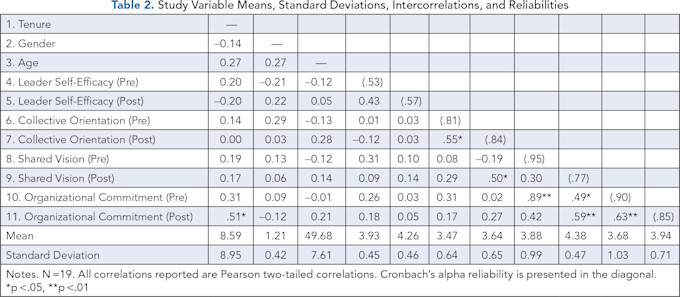
In total, 22 individuals completed the post-survey, and 19 individuals completed both the pre- and post-surveys and were included in the focal pre-post analyses. Reliabilities, means, standard deviations, and intercorrelations for all study variables are presented in Table 2. The 19 participants used in the focal analyses included nine chief medical officers, seven medical directors, and three other physician leaders. Organizational tenure ranged from one to 35 years with an average tenure of nine years. Regarding gender, 15 participants identified as men and four participants identified as women. Regarding race, 13 individuals identified as White, two as Asian, two as Middle Eastern, and two preferred not to say. Regarding ethnicity, 16 identified as Not Hispanic, one as Hispanic, and two preferred not to say.
Before testing the primary study hypotheses, we first compared post-survey scores for individuals who completed both surveys to those who completed only the post-survey. We found no significant differences in any study variables.
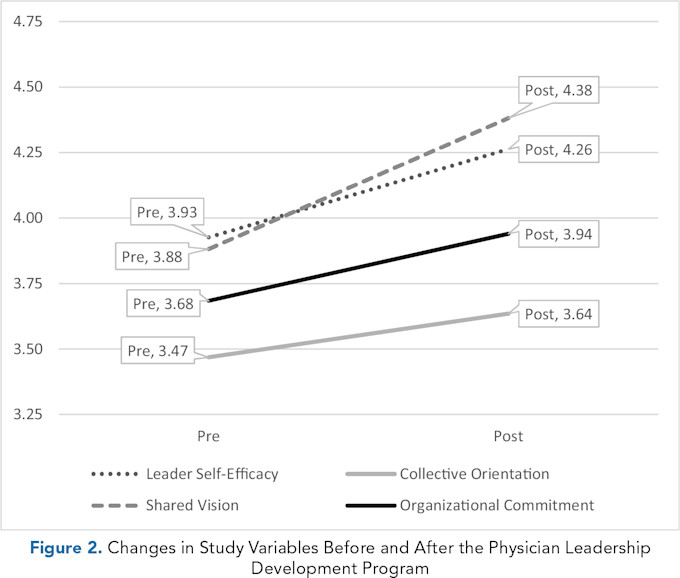
Because the hypotheses were directional, with the expectation of increases over time, one-tailed paired sample t-tests were conducted to determine the effect of the CMO Academy program on the four focal study variables. The results indicate a significant increase in leader self-efficacy scores from before the program (M = 3.95; SD = .45) to after the program (M = 4.26; SD = .45), t(18) = −3.02, p = .004.
The results also indicate a significant increase in shared vision scores from before the program (M = 3.88; SD = .99) to after the program (M = 4.38; SD = .47), t(18) = −2,27, p = .018. However, results did not indicate a significant increase in collective orientation from before the program (M = 3.47; SD = .64) and after the program (M = 3.64; SD = .65), t(18) = −1.19, p = .126, or in organizational commitment from before the program (M = 3.68; SD = 1.03) to after the program (M = 3.94; SD = .71), t(18) = −1.38, p = .092. Still, it should be noted that the change in organizational commitment is in the hypothesized direction and would be considered significant if a more lenient cutoff of p < .10 was used, as is sometimes practiced in exploratory, directional, or underpowered research.(16)
In sum, the findings confirm the expected significant improvements in leader self-efficacy and shared vision, as well as smaller, non-statistically significant improvements in collective orientation and organizational commitment (see Figure 2).
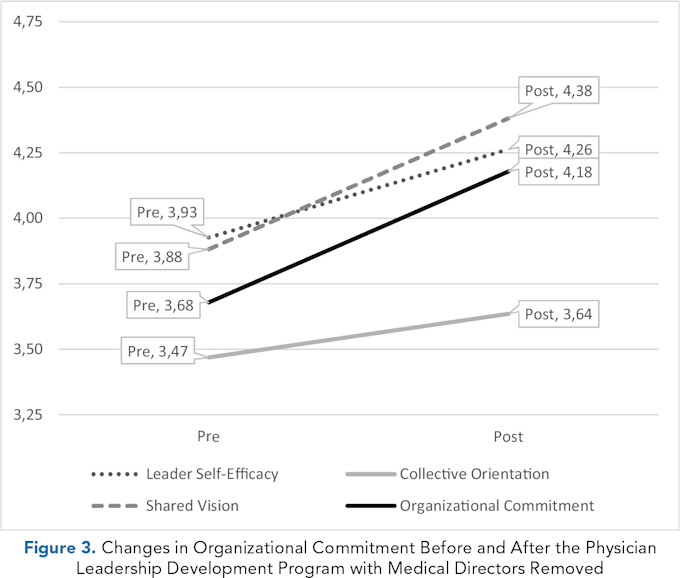
Exploratory analyses were conducted to investigate whether demographic differences were present and related to any of the findings. No significant differences were found across gender for any of the study variables, but there was a significant difference across organizational roles. Specifically, organizational commitment scores after the program were higher for chief medical officers (M = 4.19) as compared to medical directors (M = 3.41), F(2, 19) = 2.99, p = .074, suggesting that the lack of significant improvement in organizational commitment may be influenced by the unexpectedly lower post-program scores reported by medical directors. Therefore, the one-tailed paired sample t-test for organizational commitment was re-run while filtering out data from medical directors (see Figure 3), and this did in fact reveal a statistically significant increase in organizational commitment from before the program (M = 3.68; SD = 1.16) to after the program (M = 4.18; SD = .67), t(11) = −2.03, p = .034.
DISCUSSION
Following completion of the 12-month role-specific physician leadership development program, survey scores measuring leader self-efficacy, shared vision, and organizational commitment improved. The scores suggest that participants demonstrated significant improvements in leader self-efficacy and shared vision, along with smaller, positive changes in collective orientation and organizational commitment. These findings suggest that a structured, externally delivered leadership development experience can meaningfully influence physicians’ confidence in their leadership abilities and their alignment with organizational purpose.
The observed increase in leader self-efficacy is consistent with prior literature demonstrating that leadership development programs frequently enhance participants’ confidence, decision-making capacity, and perceived leadership competence.(6,12,17) This is also coherent with previous reviews that have emphasized that individual-level outcomes are among the most reliably observed effects of leadership training.(6,7)
In addition to improvements in self-efficacy, participants reported significantly greater shared vision following program completion. This finding is notable given that the program was not embedded within any single sponsoring organization. Prior studies have suggested that an increase in shared vision may be influenced by institutional proximity or organizational sponsorship.(2,4) In contrast, the externally delivered structure of the present program minimized direct organizational priming, suggesting that observed change in shared vision reflects broader cognitive and attitudinal development rather than local institutional influence. Further, these findings are consistent with prior research demonstrating the central role of shared vision in strengthening organizational commitment, of which the latter attitude also measurably increased.(14)
Role-based analyses indicated that chief medical officers experienced greater gains in organizational commitment than participants serving in medical director roles. This difference may reflect variations in role proximity to executive leadership, authority to influence organizational strategy, and opportunities to apply newly acquired leadership competencies.(8,9) CMOs may be better positioned to translate program content into organizational engagement, whereas medical directors may encounter structural or role-related constraints that limit the immediate application of leadership perspectives. These findings suggest that the participant’s title (CMO, medical director, service line director, etc.) may moderate the organizational impact of leadership development and warrant further investigation.
Collectively, the results of this study support prior work demonstrating the value of leadership development while addressing an important gap in the literature regarding post-program organizational attitudes. Whereas many evaluations focus primarily on participant satisfaction or perceived skill acquisition,(6,17) the present study demonstrates measurable changes in leadership confidence and organizational alignment using validated instruments. This contributes to a more rigorous understanding of how physician leadership development may influence both individual and organizational outcomes.
When HCOs use PLD programs to equip their physicians, they might benefit from using the results of this study as a useful guide to determine desired outcomes and allocation of resources toward those objectives. The review by Spurgeon, et al., contends that physician leadership achieves greater overall medical engagement for the organization and greater impact on organizational performance.(18) Further, when individual organizational commitment increases, and “if this is extended to a collective workforce … an organization ... has effectively increased its potential “power” to perform.”(18)
Coincidentally, physicians want defined leadership development programs, and when national physician companies have delivered such programs, the results show improved physician engagement.(19,20) With the results of this study, HCOs now have an additional option when selecting a program (or programs) to foster organizational outcomes.
By leveraging the role of senior physician leaders (e.g., CMOs) through specific role-based leadership training that provides clear learning objectives and training in specific competencies (in both management and leadership), HCOs can expect to see improved attitudes toward the parent organization. Role-specific development strengthens the key physician leader and, as a change agent, advances the dynamic between organizational administrative leadership and physician engagement.
LIMITATIONS
Several limitations should be considered when interpreting these findings. First, the sample size was modest, reflecting the limited enrollment capacity of a longitudinal, role-specific leadership program. Although statistically significant effects were observed for several outcomes, the sample size could have impacted our ability to detect smaller effects, particularly for collective orientation and organizational commitment. Similar challenges have been noted in prior evaluations of physician leadership programs.(6,7)
Second, participation in the program was voluntary, introducing the potential for self-selection bias. Individuals who elected to enroll may have been more motivated, development-oriented, or organizationally engaged than non-participants. As a result, observed changes may partially reflect pre-existing characteristics rather than program effects alone, a limitation commonly identified in leadership development research.(17)
Third, the study employed a pre-post design without a comparison group. In the absence of a control condition, causal inferences must be made cautiously. Alternative explanations, including professional maturation, concurrent organizational changes, or external leadership experiences, cannot be fully excluded.(7)
Fourth, all outcome measures relied on self-report instruments. While validated scales were used, self-report data are subject to social desirability bias and common method variance.(12-15) Participants may have reported more favorable attitudes following program completion because of the “bonding” of the experience (i.e., team building through interactive exercises), perceived expectations, or simply an increased awareness of leadership constructs.
Potentially just as confounding for interpretation is that participant physicians were at different career stages, across diverse healthcare delivery models and geographic contexts, making this (i.e., potential bonding) difficult to replicate and/or assess in future study designs.
POTENTIAL FOR FUTURE RESEARCH
Healthcare is a high-stakes environment, and developing effective leaders requires tailored programs and clear metrics to assess whether leadership behaviors improve organizational performance.(21) Additional work is needed to link PLD outcomes to downstream objective organizational metrics, including physician retention, quality performance, patient safety indicators, and financial outcomes.
Upon return to parent organizations after concluding an external PLD program, those physicians charged with leading organizational change could subsequently initiate local development programs with local physician leaders and measure self-reported assessments of organizational commitment and shared vision, as well as the aforementioned metrics. Establishing these connections would strengthen the evidence base for investment in external role-based PLD. Further, gathering evidence that instilling senior physician leaders (i.e., CMOs) with critical training and development will foster subsequent organizational outcomes, particularly at the physician enterprise level, would be of great importance to HCOs and healthcare in general.
Comparative studies evaluating externally delivered versus institution-based leadership programs would further clarify the relative advantages and limitations of each model. Such research could inform organizational decisions regarding program design, resource allocation, and scalability.(2,4) As Lyons stated, “Educational methods appear to be more important for organizational outcomes than specific curriculum content. Improving evaluation design will allow educators and evaluators to more effectively understand factors that are reliably associated with organizational outcomes of leadership development.”(22) Also, understanding how curriculum design influences leadership effectiveness remains an important area of inquiry.(3)
Future investigations should directly compare role-specific leadership curricula with more generalized physician leadership programs to determine what impacts targeted training yields (compared to general development) regarding organizational outcomes. Finally, research examining the relationship between leadership development participation and progression into senior executive roles may help clarify how structured training contributes to the development of future healthcare leaders and organizational change agents.(8,9)
References
Hoff T, Lee DR, Prout K. Organizational commitment among physicians: A systematic literature review. Health Serv Manage Res. 2021;34(2):99–112. https://doi.org/10.1177/0951484820952307 .
Scheinbart L, Hertling M, Wildman J. Improving organizational commitment through inter-professional leadership development programs. Physician Leadersh J. 2024;11(5):5–11. https://doi.org/10.55834/plj.4829940553 .
Leskiw S, Singh P. Leadership development: learning from best practices. Leadersh Organ Dev J. 2007;28(5):444–464. https://doi.org/10.1108/01437730710761742 .
Hertling M. Physicians must lead! a comparative study of two approaches to physician leadership development. Diss. Exec. Doctorate in Business Administration Program. Rollins College. 2019. 1-111. https://scholarship.rollins.edu/cgi/viewcontent.cgi?article=1036&context=dba_dissertations
Hertling M. Study: approaches to leadership training at top nonprofit hospitals. Physician Leader J. 2018;5(6):28–34.
Frich J, Brewster A, Cherlin E, Bradley E. Leadership development programs for physicians: a systematic review. J Gen Intern Med. 2015;30(5): 656–674. https://doi.org/10.1007/s11606-014-3141-1 .
Debets M, Jansen I, Lombarts K, Kuijer Siebelink W, Kruijthof K, et al. Linking leadership development programs for physicians with organization‑level outcomes: a realist review. BMC Health Serv Res. 2023;23(1):783. https://doi.org/10.1186/s12913-023-09811-y .
Hlavin J. CMO experiences: a rudimentary case report. Physician Leadersh J. 2019; 12(5):43–49.
Onyango R, Baker MC, Faerberg J. Evolution of the chief medical officer role in teaching hospitals and health systems. J Healthc Manag. 2023;68(2):121–131. https://doi.org/10.1097/JHM-D-22-00097 .
Chief Medical Officer Academy. American Association for Physician Leadership. https://www.physicianleaders.org/cmo-academy.
Bruner JS. The Process of Education. Harvard University Press;1960. https://doi.org/10.4159/9780674028999 .
Ladegard G, Gjerde S. Leadership coaching, leader role-efficacy, and trust in subordinates. A mixed methods study assessing leadership coaching as a leadership development tool. Leadersh Q. 2014;25(4): 631–646. https://doi.org/10.1016/j.leaqua.2014.02.002 .
Driskell J, Salas E, Hughes S. Collective orientation and team performance: development of an individual differences measure. Hum Factors. 2010;52(2):316–328. https://doi.org/10.1177/0018720809359522 .
Chai D, Hwang S, Joo B. Transformational leadership and organizational commitment in teams: the mediating roles of shared vision and team-goal commitment. Perform Improve Q. 2017;30(2):137–158. https://doi.org/10.1002/piq.21244 .
McGee G, Ford R. Two (or more?) dimensions of organizational commitment: reexamination of the affective and continuance commitment scales. J Applied Psychol. 1987;72(4): 638–641. https://doi.org/10.1037//0021-9010.72.4.638 .
Schumm W. Determining statistical significance (alpha) and reporting statistical trends: controversies, issues, and facts. Compr Psychol. 2013; 2(Art.10). https://doi.org/10.2466/03.CP.2.10 .
Phillipson J, Pinto AC, Lyons O. Leadership training in healthcare: a systematic umbrella review. BMJ Lead. 2025;9(4):349-359. https://doi.org/10.1136/leader-2025-001269 .
Spurgeon P, Long P, Clark J, Daly F. Do we need medical leadership or medical engagement? Leadersh Health Serv. 2015;28(3):173–184. https://doi.org/10.1108/LHS-03-2014-0029 .
Liang C, Menaker S, Mahoney M. Physician Perceptions of Administrative Leadership Development Post-COVID-19. Physician Leadersh J. 2023;10(4):18–26. https://doi.org/10.55834/plj.4555925887
Perry J, Mobley F, Brubaker M. Most doctors have little or no management training, and that’s a problem. Harvard Business Review. December 15, 2017. https://hbr.org/2017/12/most-doctors-have-little-or-no-management-training-and-thats-a-problem
Hertling M, Smith-Jentsch, K. Measuring leadership growth: metrics as a part of physician leadership development. Physician Leadersh J. 2026;3(1):45–47. https://doi.org/10.55834/plj.9588106623 .
Lyons O, George R, Galante JR. Evidence-based medical leadership development: a systematic review. BMJ Leader. 2021;5:206–213. https://doi.org/10.1136/leader-2020-000360 .