
On November 7, 2022, Harris Health System received a request from the Houston Health Department to accept a patient under investigation for a concern related to Ebola virus disease (EVD) in a patient who had returned from Uganda in the previous 21 days. The patient’s chief complaints were fever and fatigue. Our health system had approximately eight hours’ notice to prepare for the patient’s arrival to our Ben Taub Hospital Emergency Department. Harris Health’s Ben Taub Hospital is a Level I trauma center with 402 licensed acute-care beds and is a teaching affiliate for Baylor College of Medicine. It was notable that an outbreak of EBV was confirmed in western Uganda from September 20, 2022 to January 11 2023.(1) According to the World Health Organization, during that outbreak there were 165 cases of EVD, with 55 confirmed deaths, and there were no known cases in the United States. Our goal was to ensure the safety of our patient, our healthcare workers, and our community while maintaining business as usual and minimizing panic.
Due to the gravity of the situation, a safety huddle was immediately called to bring key stakeholders together and to prepare to set up a hospital incident command system (HICS). HICS is the methodology used by health systems to deal with emergency situations while ensuring continued operations during crises such as hurricanes, floods, fire, mass casualty, and pandemics. The HICS is structured to include several important roles, including an incident commander to lead the response, a public information officer, a liaison officer, a safety officer, a logistics chief, a planning chief, a finance chief, and an operations chief. The number of people involved in the response may vary, and specific roles may be combined, depending on the size of the hospital or the crisis at hand. We identified all officers and chiefs but combined the roles of finance and operations chief into one role. The HICS ensured coordination of care, allocation of supplies, and clear communication, both internally in the organization and externally to stakeholders, throughout the crisis.(2)
At the HICS center, we performed frequent safety huddles and assigned tasks from each department with clear deliverables with specific timelines. All were asked to report back to the incident command center. The teams were encouraged to work together collaboratively for the greater good of the patient. We answered all questions to the best of our ability and with the information that was available to us at the time.
Ebola virus disease is a rare disease with a fatality rate ranging from 20% to 90%.(3) Symptoms can include fever, headache, muscle pain, weakness, fatigue, diarrhea, vomiting, bleeding, or bruising. Ebola virus disease is highly contagious. It is transmitted to people from wild animals and spreads in the human population by human-to-human transmission through body fluids. It is not usually spread through the air or casual contact. The incubation period ranges from 2 to 21 days before people show symptoms. Healthcare workers are at high occupational risk when taking care of patients with EVD without proper personal protective equipment (PPE).(4) The gold standard test used to diagnose EVD is polymerase chain reaction looking for Ebola virus RNA in the blood. The main treatment is supportive therapy, including intravenous fluids and oxygen while also managing the symptoms of vomiting or diarrhea. The FDA recently approved two intravenous monoclonal antibody treatments for EVD, Inmazeb, and Ebanga.(5)
Our state’s history with EVD had a further impact on the psyche of our team. On September 30, 2014, EVD was diagnosed in the United States for the first time when a Liberian national tested positive for EVD in Dallas, Texas.6 The patient died on October 8, 2014, but two nurses who treated him contracted EVD and survived. The CDC reviewed the case in detail and noted that one of the factors that contributed to the nurses’ infection was a breach in the PPE donning and doffing protocol. A lawsuit was filed against the hospital where the nurses became infected; it was later settled out of court.(6)
A crisis is defined as “a significant threat to operations of an organization that can have negative consequences if not handled properly.”(7) A crisis can threaten the organization through three possible mechanisms: 1) public safety; 2) financial loss; and 3) reputational loss.
Our team had little time to manage this new crisis that had arrived at our doorstep. Given the transmissibility and high fatality rate of EVD, the situation required us to set into motion a plan to manage this crisis to minimize the potential danger to public safety. A lapse in any of the protocols might also lead to a potential loss of our reputation in the eyes of our employees and the public at large.
How did we prepare to receive a potential EVD patient under investigation while ensuring the safety of this patient, the other healthcare workers, and our community? The leadership team applied Kotter’s eight-step change management model to help manage through the crisis and engage our team (Table 1).(8)
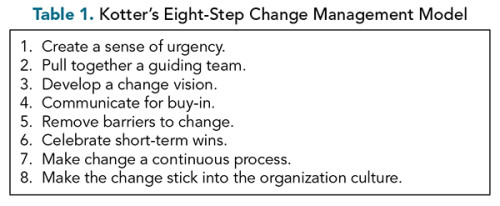
The first step in change management is to create a sense of urgency by having a burning platform. The sense of urgency was palpable, given the fact that the EVD patient under investigation was coming our way in about eight hours.
The next step, pull together a guiding team, involved multiple levels, including the nursing director, pharmacy, laboratory, infection preventionists, central supply chain leadership, emergency medicine physician leadership, infectious disease specialists, and hospital administrative leadership. We involved our emergency preparedness specialists to help us manage the operations of the command center and provide further subject matter expertise on the management of the crisis.
We needed to develop a change vision. The goal was to set up an Ebola virus containment area in the hospital emergency department where the patient could be placed. We wanted to ensure the maximum safety for our patient under investigation, our employees, and our other patients in the area. Our vision was to ensure that all CDC Ebola guidelines were followed and that our nurses and physicians felt safe taking care of the patient. This was accomplished through just-in-time education, training, communication, and validation of competency on proper donning and doffing of PPE.
Communication for buy-in was crucial. This allowed the team to express their fears, their anger, and their concerns regarding having a patient under investigation in our hospital. In addition, getting communication feedback from the team allowed us to optimize our care plans and review the processes that we put into place. Our communication team created a memo that was sent out to the entire health system to provide high-level communication of the facts and also to minimize rumors among our employees. Communication is very important for both internal and external stakeholders. There was constant communication between the front-line employees, the incident command center, the hospital administrative team, the corporate office, and the city and county public health departments.
We created a volunteer army to empower the front-line groups to remove barriers to change. We asked the different teams to create small subgroups to develop action plans in their respective areas of responsibilities and asked them to report back every one to two hours to the incident command center to give the latest updates. We had a running checklist in the command center on the white board to allow for accountability and to ensure proper results. At the incident command center, we worked collectively to create a checklist of all the actions needed, by department. The leadership spent time removing the obstacles that prevented our progress to ensure an ideal outcome. Our planning team included key members from system executive leadership, hospital executive leadership, nursing, physicians, supply chain management, infectious disease service, infection prevention, emergency management, hazardous material management, facility engineering, safety, security, environmental services, communications, laboratory, information technology, and local health department (Table 2).

We also built on the change by celebrating the short-term wins when the patient arrived and noted how well prepared we were. We made change a continuous process by keeping the command center open while maintaining periodic debriefs and updates throughout the day. We spent time noting what was going well, what was not going well, and what were the learning opportunities. We recognized the team by rounding on them, praising them, ensuring they had adequate breaks, providing them meals, and allowing them to report out issues that concerned them.
Ebola ultimately was ruled out based on two separate tests, and an alternative diagnosis was made. The patient stayed with us for five days. There was a collective sense of pride as we maintained as top priority the safety of our patient and employees during this time while maintaining great morale and minimizing panic.
Although the patient ultimately was not diagnosed with EVD, the health team showed its immediate ability to be successful in managing this crisis in an effective way. Furthermore, to anchor the change into the organizational culture, we organized a final debrief a week after the patient was discharged to understand what the learning opportunities were. This allowed us to develop a written policy and procedure on receiving a patient with EVD at our health system.
There were several key takeaway lessons on crisis management that can be summarized by remembering the five Cs based on the literature on crisis management:(9-11)
Get comfortable with chaos. In crisis you often must act without full information, as we did with this patient under investigation for possible EVD. The incident required us to set up an incident command center, develop priorities, and move forward with actions and learn quickly from mistakes. Having an action plan is important, but being adaptable and willing to pivot if needed is even more crucial. A leader must be able to be agile and sometimes live with ambiguity. Information may change from one moment to the next, and leaders must be willing to recognize their blind spots. Bringing outside experts to provide further guidance on a situation can be helpful. We engaged our front-line workers, our infectious disease physicians, our emergency medicine physicians, and the Houston Department of Public Health, as well as the CDC to help guide us through this complex situation.
Communication is key. You cannot overcommunicate, either internally and externally, through multiple channels. Internal and external communication are equally important. We held regular meetings by telephone, in person, or by Webex as early as possible to prevent miscommunication. The executive team also rounded periodically through the emergency department and floors of the hospital to show support, monitor progress, and answer questions and clear up any rumors. Specific concerns and needs were funneled through the incident command center and were addressed promptly to ensure coordination. The communication department helped take a lead on the communications for external stakeholders by providing daily memos to the rest of the health system on the progress we were making.
Compassion is crucial. Despite all the ongoing stress, it is important to remember that compassion for your front-line healthcare workers is a priority. Rounding on your employees to get their feedback, providing words of support, celebrating early success, encouraging breaks, and even bringing them snacks can all be helpful ways to demonstrate compassion. Maya Angelou said it best: “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.”
The community as a whole needs to be emphasized. Nothing can be more powerful than emphasizing the “one community” approach around a common goal. Each department carried out its own duties separately to make our united plan run smoothly and safely. However, each department reported out at the incident command center the progress made, allowing each department to show their pride in their work. The regular meetings provided a way to connect together on a personal level as a team by providing a social support to help everyone manage the stress which ultimately allowed us to be united as one.
Checklists are necessary to help ensure a smooth and reliable operation. We developed one major checklist at the incident command center to ensure that we were closing the loop on the action plans and to provide further guidance on next steps. This checklist served as the agenda for the daily huddles. The CDC’s interim guidance for Ebola helped us to also develop a preparedness checklists for patient placement, transportation, and laboratory testing.(12) Infection Prevention developed checklists using the CDC’s PPE training to make sure that all staff were trained and validated on donning and doffing to the same standards.(13) Despite ongoing supply chain issues and challenges of products on backorder, we were fortunate to have secured sufficient quantities of all necessary PPE used for the patient under investigation and for training.
Martin Luther King Jr., summed up the principles of leadership best when he said, “The ultimate measure of a man is not where he stands in the moments of comfort, but where he stands at times of challenge and controversy.” Based on our experience with managing this crisis, we confirm this adage to be true. The combination of leadership from the executive team, multidisciplinary involvement, clear communication, and using the HICS structure ultimately ensured our success: the safety of patients, healthcare workers, and the community at large while maintaining the operation of the hospital, minimizing panic, and ensuring team morale. There was an agile collaborative multidisciplinary response with clear accountability. The potential for rumors, chaos, and information overload is a concern during a crisis, but it can be overcome via authentic transparent leadership principles reviewed here. The experience of managing the crisis drew our team closer and made us even more confident in both the resilience and agility of the Ben Taub Hospital and the Harris Health System. We stand on guard prepared to manage the next crisis—which is sure to come—armed with the confidence and the knowledge that we will prevail.
References
World Health Organization 2022, Ebola Uganda, 2022. www.who.int/emergencies/situations/ebola-uganda-2022 . Accessed March 25, 2023.
Shooshtari S, Tofighi S, Abbasi S. Benefits, barriers, and limitations on the use of Hospital Incident Command System. J Res Med Sci. 2017;22:36. https://doi.org/10.4103/1735-1995.202146
Sprecher A. Understanding the key to outbreak control—Sudan Virus Disease in Uganda. N Engl J Med. 2022;387:2393-2395. https://doi.org/10.1056/NEJMp2213975
Hewlett AL, Varkey JB, Smith PW, Ribner BS. Ebola virus disease: preparedness and infection control lessons learned from two biocontainment units. Curr Opin Infect Dis. 2015;28:343-348. https://doi.org/10.1097/QCO.0000000000000176 PMID: 26098504; PMCID: PMC4743738.
Ebola disease. Centers for Disease Control and Prevention. February 26, 2021. www.cdc.gov/vhf/ebola/treatment/index.html . Accessed March 31, 2023.
Courage KH. How did a Dallas nurse catch Ebola? Scientific American. October 15, 2014. www.scientificamerican.com/article/how-did-a-dallas-nurse-catch-ebola/ Accessed March 25, 2023.
Crisis management and communications. Institute for Public Relations. October 30, 2007. https://instituteforpr.org/crisis-management-and-communications/ Accessed March 25, 2023.
Kotter JP. Leading change: why transformation efforts fail. Harvard Business Review.1995; May-June. https://hbr.org/1995/05/leading-change-why-transformation-efforts-fail-2 . Accessed March 25, 2023.
Augustine NR. Crisis management: managing the crisis you tried to prevent. Harvard Business Review. 1995;November-December.
Kerrissey MJ, Edmondson AC. Crisis management: what good leadership looks like during this pandemic. Harvard Business Review. 2020;April.
Nichols C, Chatterjee HS, Trendler C. Career coaching: 4 behaviors that help leaders manage a crisis. Harvard Business Review. 2020;April.
Ebola disease. Centers for Disease Control and Prevention. October 7, 2022. www.cdc.gov/vhf/ebola/clinicians/emergency-services/emergency-department-training.html . Accessed March 25, 2023.
Guidance for donning and doffing personal protective equipment (PPE) during management of patients with Ebola virus disease in U.S. hospitals. Centers for Disease Control and Prevention. October 7, 2022. www.cdc.gov/vhf/ebola/hcp/ppe-training/index.html . Accessed March 25, 2023.